Fill in a Valid Sports Physical Form
Document Sample
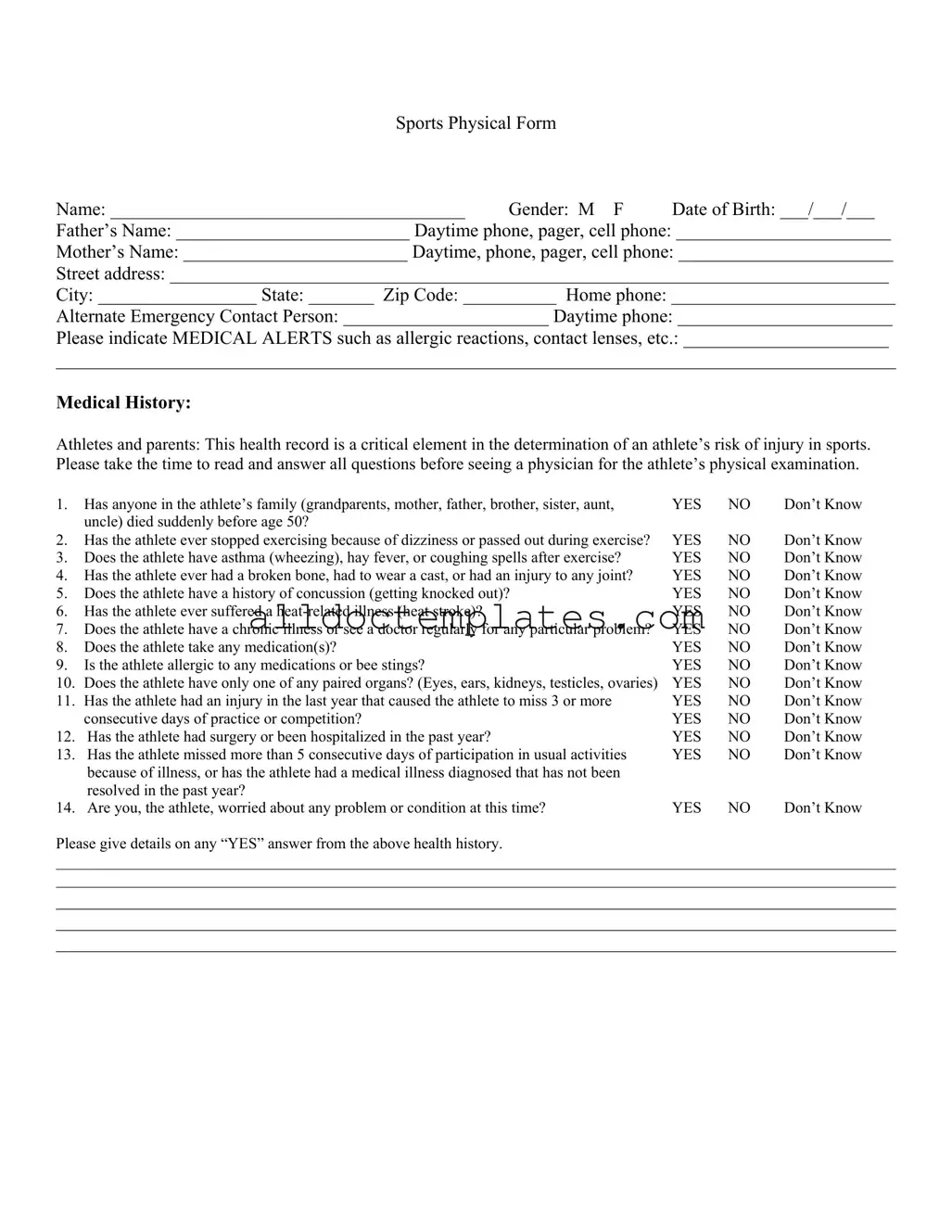
Sports Physical Form
Name: ______________________________________ Gender: M F Date of Birth: ___/___/___
Father’s Name: _________________________ Daytime phone, pager, cell phone: _______________________
Mother’s Name: ________________________ Daytime, phone, pager, cell phone: _______________________
Street address: _____________________________________________________________________________
City: _________________ State: _______ Zip Code: __________ Home phone: ________________________
Alternate Emergency Contact Person: ______________________ Daytime phone: _______________________
Please indicate MEDICAL ALERTS such as allergic reactions, contact lenses, etc.: ______________________
__________________________________________________________________________________________
Medical History:
Athletes and parents: This health record is a critical element in the determination of an athlete’s risk of injury in sports. Please take the time to read and answer all questions before seeing a physician for the athlete’s physical examination.
1. |
Has anyone in the athlete’s family (grandparents, mother, father, brother, sister, aunt, |
YES |
NO |
Don’t Know |
|
uncle) died suddenly before age 50? |
|
|
|
2. |
Has the athlete ever stopped exercising because of dizziness or passed out during exercise? |
YES |
NO |
Don’t Know |
3. |
Does the athlete have asthma (wheezing), hay fever, or coughing spells after exercise? |
YES |
NO |
Don’t Know |
4. |
Has the athlete ever had a broken bone, had to wear a cast, or had an injury to any joint? |
YES |
NO |
Don’t Know |
5. |
Does the athlete have a history of concussion (getting knocked out)? |
YES |
NO |
Don’t Know |
6. |
Has the athlete ever suffered a |
YES |
NO |
Don’t Know |
7. |
Does the athlete have a chronic illness or see a doctor regularly for any particular problem? |
YES |
NO |
Don’t Know |
8. |
Does the athlete take any medication(s)? |
YES |
NO |
Don’t Know |
9. |
Is the athlete allergic to any medications or bee stings? |
YES |
NO |
Don’t Know |
10. |
Does the athlete have only one of any paired organs? (Eyes, ears, kidneys, testicles, ovaries) |
YES |
NO |
Don’t Know |
11. |
Has the athlete had an injury in the last year that caused the athlete to miss 3 or more |
YES |
NO |
Don’t Know |
|
consecutive days of practice or competition? |
YES |
NO |
Don’t Know |
12. Has the athlete had surgery or been hospitalized in the past year? |
YES |
NO |
Don’t Know |
|
13. Has the athlete missed more than 5 consecutive days of participation in usual activities |
YES |
NO |
Don’t Know |
|
|
because of illness, or has the athlete had a medical illness diagnosed that has not been |
|
|
|
|
resolved in the past year? |
|
|
|
14. |
Are you, the athlete, worried about any problem or condition at this time? |
YES |
NO |
Don’t Know |
Please give details on any “YES” answer from the above health history.
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
PHYSICAL EXAM – TO BE COMPLETED BY PHYSICIAN
Height __________ |
Weight __________ |
Pulse __________ |
Blood Pressure __________ |
Vision: R _____ / _____ uncorrected R _____ / _____ corrected |
L _____ / _____ uncorrected L _____ / _____ corrected |
||
Normal |
Abnormal Findings |
1.Eyes
2.Ears, Nose, Throat
3.Mouth & Teeth
4.Neck
5.Cardiovascular
6.Chest & Lungs
7.Abdomen
8.Skin
9.
10.Muskuloskeletal: ROM, strength, etc.
a.neck
b.spine
c.shoulders
d.arms/ hands
e.hips
f.thighs
g.knees
h.ankles
i.feet
11.Neuromuscular
Initials
Please Print/ Stamp
Physician’s Name ___________________________________________________________________________________
Street Address _____________________________________________________________________________________
City, State, Zip Code ________________________________________________________________________________
Telephone _________________________________________________________________________________________
I certify that I have examined this athlete and found him/her medically qualified to participate in sports. I also certify that I am a licensed medical physician, physician’s assistant, or family nurse practitioner. (Doctor of Chiropractic Medicine is not satisfactory.)
Physician Signature __________________________________________________________ Date __________________
PARTICIPATION RESTRICTIONS: _________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Document Information
| Fact Name | Description |
|---|---|
| Form Purpose | The Sports Physical form assesses an athlete's health and readiness for sports participation. |
| Required Information | It collects personal details such as name, gender, date of birth, and contact information for parents or guardians. |
| Medical Alerts | Parents must indicate any medical alerts, including allergies or special conditions, to ensure athlete safety. |
| Health History | The form includes a series of questions regarding the athlete's medical history, such as previous injuries or chronic illnesses. |
| Physical Exam | A licensed physician must complete the physical examination section, documenting the athlete's height, weight, and vital signs. |
| Physician Certification | The physician must certify that the athlete is medically qualified to participate in sports, ensuring compliance with health standards. |
| State-Specific Forms | Some states have specific requirements for sports physicals, governed by local laws. Always check state regulations. |
| Participation Restrictions | Any restrictions on the athlete's participation must be clearly noted by the physician on the form. |
Sports Physical - Usage Guidelines
Completing the Sports Physical form is an important step in ensuring that an athlete is ready to participate in sports activities. The form collects essential information about the athlete's medical history and current health status, which will be reviewed by a physician during the physical examination. Follow these steps to fill out the form accurately.
- Begin with personal information: Write the athlete's name, gender, and date of birth at the top of the form.
- Provide parental information: Fill in the names and daytime contact numbers for both the father and mother.
- Enter the athlete's address: Include the street address, city, state, and zip code.
- List the home phone number: Write the home phone number of the athlete.
- Emergency contact: Identify an alternate emergency contact person and provide their daytime phone number.
- Note any medical alerts: Indicate any medical alerts such as allergies or the use of contact lenses.
- Complete the medical history section: Answer each question with "YES," "NO," or "Don’t Know." Be honest and thorough.
- Provide details for "YES" answers: If any questions were answered "YES," provide further details in the space provided.
- Physician's examination section: Leave this section blank for the physician to complete during the physical examination.
- Physician's information: After the examination, the physician will fill out their name, address, and contact number.
- Signature and date: The physician will sign and date the form, certifying that the athlete is medically qualified to participate in sports.
- Participation restrictions: If applicable, the physician will note any participation restrictions at the end of the form.
Common PDF Forms
Hub Texas - Each entry supports the verification of membership status and transaction legitimacy.
For those considering a horse purchase or sale, it's crucial to have the proper documentation in place. The Colorado Horse Bill of Sale form not only ensures a legal transfer of ownership but also provides a reliable record of the transaction. To make the process easier, you can find a suitable template at Colorado PDF Templates, which outlines all necessary details to protect both parties involved.
Rochdale Village Income Requirements - Benefit from on-site security measures ensuring safety and peace of mind for all residents.
Irs 1040 Form - The IRS provides online tools to assist in filling out the 1040 form.
Dos and Don'ts
When filling out the Sports Physical form, it is important to approach the task with care and attention to detail. Here are four key things to do and not do:
- Do ensure accuracy: Fill out all sections of the form with correct information, especially personal details like name, date of birth, and contact information.
- Do provide complete medical history: Answer all medical history questions honestly and thoroughly. This information is crucial for assessing the athlete's health risks.
- Do ask for assistance if needed: If you are unsure about how to answer a question, seek help from a parent, guardian, or medical professional.
- Do keep a copy of the form: After submission, retain a copy for your records. This can be useful for future reference.
- Don't rush through the form: Take your time to read each question carefully. Incomplete or rushed answers can lead to misunderstandings.
- Don't omit important information: Failing to disclose medical alerts or past injuries could jeopardize the athlete's safety during sports activities.
- Don't use unclear language: Write clearly and legibly. Avoid abbreviations that may confuse the reader.
- Don't forget to sign: Ensure that the physician's signature is included, as this validates the physical examination.
Common mistakes
-
Incomplete Personal Information: Failing to fill out all sections, such as the athlete’s name, date of birth, or contact information, can lead to delays or complications in processing the form.
-
Missing Medical Alerts: Not indicating any medical alerts, like allergies or existing conditions, may put the athlete at risk during physical activities.
-
Neglecting Family Medical History: Skipping questions about family medical history can overlook important hereditary risks that may affect the athlete's health.
-
Inconsistent Answers: Providing conflicting answers to similar questions can confuse the reviewing physician and delay the evaluation process.
-
Overlooking Recent Injuries: Failing to disclose recent injuries or surgeries can lead to inadequate assessments and increase the risk of further injury.
-
Ignoring Medication Information: Not mentioning current medications can pose serious health risks, especially if the athlete experiences an adverse reaction during sports.
-
Forgetting Emergency Contact Details: Omitting an alternate emergency contact can create complications in urgent situations where immediate communication is necessary.
-
Not Providing Detailed Explanations: When answering "YES" to health history questions, failing to provide additional details can leave the physician with incomplete information.
-
Skipping the Physician’s Section: Not ensuring that the physician completes their section, including their signature and date, can invalidate the form.