Fill in a Valid Medication Error Form
Document Sample
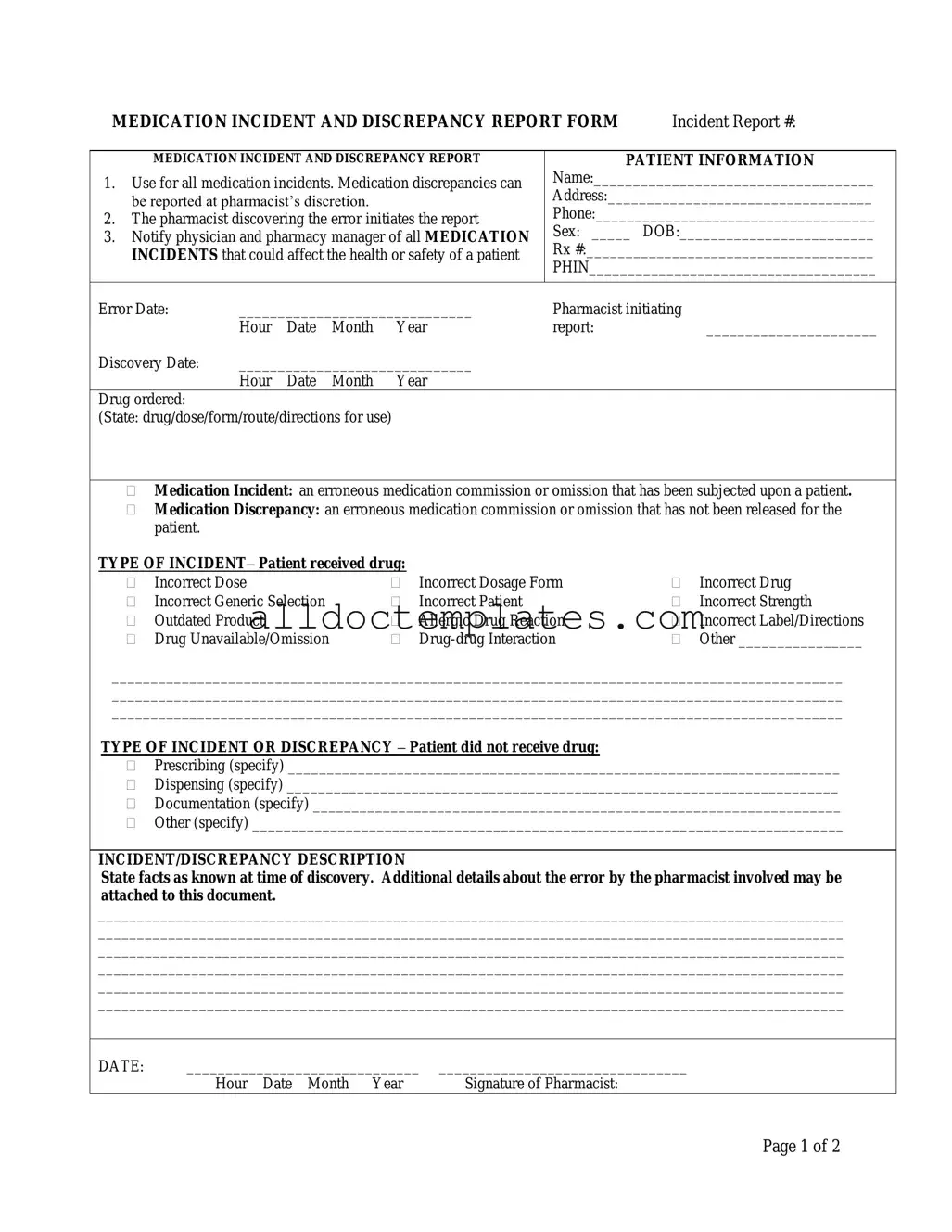
MEDICATION INCIDENT AND DISCREPANCY REPORT FORM |
Incident Report #: |
MEDICATION INCIDENT AND DISCREPANCY REPORT
1.Use for all medication incidents. Medication discrepancies can be reported at pharmacist’s discretion.
2.The pharmacist discovering the error initiates the report
3.Notify physician and pharmacy manager of all MEDICATION INCIDENTS that could affect the health or safety of a patient
PATIENT INFORMATION
Name:____________________________________
Address:__________________________________
Phone:____________________________________
Sex: _____ DOB:_________________________
Rx #:_____________________________________
PHIN_____________________________________
Error Date: |
______________________________ |
Pharmacist initiating |
|
|||
|
Hour |
Date |
Month |
Year |
report: |
______________________ |
Discovery Date: |
______________________________ |
|
|
|||
|
Hour |
Date |
Month |
Year |
|
|
Drug ordered: |
|
|
|
|
|
|
(State: drug/dose/form/route/directions for use) |
|
|
|
|||
Medication Incident: an erroneous medication commission or omission that has been subjected upon a patient.
Medication Discrepancy: an erroneous medication commission or omission that has not been released for the patient.
TYPE OF INCIDENT– Patient received drug: |
|
|
|
||
|
Incorrect Dose |
|
Incorrect Dosage Form |
|
Incorrect Drug |
|
Incorrect Generic Selection |
|
Incorrect Patient |
|
Incorrect Strength |
|
Outdated Product |
|
Allergic Drug Reaction |
|
Incorrect Label/Directions |
|
Drug Unavailable/Omission |
|
|
Other ________________ |
|
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
TYPE OF INCIDENT OR DISCREPANCY – Patient did not receive drug:
Prescribing (specify) _______________________________________________________________________
Dispensing (specify) _______________________________________________________________________
Documentation (specify) ____________________________________________________________________
Other (specify) ____________________________________________________________________________
INCIDENT/DISCREPANCY DESCRIPTION
State facts as known at time of discovery. Additional details about the error by the pharmacist involved may be attached to this document.
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
DATE: |
______________________________ |
________________________________ |
|
Hour Date Month Year |
Signature of Pharmacist: |
Page 1 of 2
CONTRIBUTING FACTORS
(To be completed by pharmacist responsible)
|
Improper patient identification |
Misread/misinterpreted drug order (include verbal orders) |
|
|
Incorrect transcription |
|
Drug unavailable |
Lack of patient counselling |
|
Other |
|
|
DATE: |
______________________________ |
__________________ |
|
|
||||
|
|
Hour Date Month Year |
Signature |
|
|
|
|||
|
NOTIFICATION – Complete the following information according to Standards of Practice. |
||||||||
1. |
Patient notified: |
|
|
|
|
|
|
|
|
|
|
|
___________________________ |
|
|||||
|
|
|
Hour |
Date |
Month |
Year |
|||
2. |
Physician notified: ____ |
______________________________ |
|
||||||
|
|
Yes/No |
Hour |
Date |
Month |
Year |
|||
|
|
|
|
|
|
|
|
|
|
|
SEVERITY |
|
|
|
|
|
|
|
|
|
|
None |
|
No change in patient’s condition: no medical intervention |
|||||
|
|
Minor |
|
|
|
required |
|
|
|
|
|
Major |
|
Produces a temporary systemic or localized response: does |
|||||
|
|
|
|
|
|
not cause ongoing complications |
|||
|
|
|
|
Requires immediate medical intervention |
|||||
|
OUTCOME OF INVESTIGATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Problem Identification |
|
|
|
Action |
|
|
|
|
|
|
Lack of knowledge |
|
|
Education provided |
||||
|
|
Performance problem |
|
|
Policy/procedure changed |
||||
|
|
Administration problem |
|
|
System changed |
|
|
||
|
|
Other |
|
|
Individual awareness |
||||
|
|
|
|
|
Group awareness |
||||
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|||||
|
RESOLUTION OF PROBLEM THAT RESULTED IN THE ERROR BEING MADE: |
||||||||
|
|
|
|
|
|
|
|
||
|
Signature: |
Date: |
Signature: |
Date: |
|||||
|
(Pharmacist filling out the form) |
|
|
|
(Pharmacy Manager) |
||||
PHARMACY USE ONLY
Page 2 of 2
Document Information
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is used for reporting all medication incidents and discrepancies that occur in a pharmacy setting. |
| Initiation of Report | The pharmacist who discovers the medication error is responsible for initiating the report. |
| Notification Requirements | All medication incidents that may impact patient health or safety must be reported to the physician and pharmacy manager. |
| Patient Information Section | The form requires essential patient details such as name, address, phone number, sex, date of birth, and prescription number. |
| Types of Incidents | Incidents can include incorrect dosage, wrong drug, allergic reactions, and more. Each type must be clearly indicated on the form. |
| Severity Levels | The form includes a section to classify the severity of the incident, ranging from no change in condition to requiring immediate medical intervention. |
| Contributing Factors | Pharmacists must identify contributing factors such as improper patient identification or misinterpretation of drug orders. |
| Follow-Up Actions | After an incident, actions may include providing education, changing policies, or improving system processes to prevent future errors. |
| State-Specific Regulations | For state-specific forms, it is essential to reference the applicable governing laws related to medication error reporting. |
Medication Error - Usage Guidelines
Completing the Medication Error form is an important step in ensuring patient safety and addressing medication discrepancies. This process requires careful attention to detail and accuracy. After filling out the form, it will be reviewed by the relevant parties, including the pharmacy manager, to determine the necessary actions and follow-up procedures.
- Locate the form: Obtain the Medication Incident and Discrepancy Report Form from your pharmacy's designated area.
- Fill in the incident report number: Write down the Incident Report # at the top of the form.
- Provide patient information: Enter the patient's name, address, phone number, sex, date of birth (DOB), prescription number (Rx #), and patient health identification number (PHIN).
- Document the error date: Indicate the date the medication error occurred.
- Identify the pharmacist: Write the name of the pharmacist initiating the report and the date of discovery.
- Specify the drug ordered: Clearly state the drug, dosage, form, route, and directions for use.
- Select the type of incident: Mark the appropriate box to indicate whether it was a medication incident or discrepancy, and provide details if necessary.
- Detail the type of incident or discrepancy: Indicate whether the patient received the drug incorrectly or did not receive the drug, specifying the nature of the issue.
- Describe the incident: Provide a detailed account of the incident as known at the time of discovery. Include any relevant facts or attach additional details if necessary.
- Complete contributing factors: Check all applicable factors that contributed to the error.
- Document notifications: Record the date and time when the patient and physician were notified about the incident.
- Assess severity: Mark the appropriate level of severity regarding the patient's condition.
- Outline follow-up actions: Specify any actions taken to resolve the problem and improve processes to prevent future occurrences.
- Sign the form: Ensure that both the pharmacist filling out the form and the pharmacy manager sign and date the document.
Common PDF Forms
1099 Nec Fillable Form - The form includes spaces for state income tax deductions as well.
The Colorado Articles of Incorporation form is a legal document that establishes a corporation in the state of Colorado. This form outlines essential details about the corporation, including its name, purpose, and structure, making it an important resource for entrepreneurs. For more information, you can visit Colorado PDF Templates, which provides helpful insights on how to complete the form properly. Filing this document is a crucial step for anyone looking to start a business in Colorado.
Tax Form Schedule C - The Profit and Loss form highlights the relationship between income and expenditures.
Dos and Don'ts
When filling out the Medication Error form, it is crucial to adhere to best practices to ensure accuracy and compliance. Below are essential dos and don’ts:
- Do use the form for all medication incidents, regardless of their severity.
- Do ensure that the pharmacist discovering the error initiates the report.
- Do promptly notify the physician and pharmacy manager of any incidents that could impact patient safety.
- Do provide clear and concise details about the incident in the description section.
- Don't omit any relevant patient information, such as name and contact details.
- Don't delay in reporting the incident; timely notification is essential.
- Don't forget to document the contributing factors accurately.
- Don't leave any sections of the form incomplete; ensure all fields are filled out.
Common mistakes
-
Incomplete Patient Information: Failing to provide all necessary details about the patient can lead to confusion and complicate follow-up actions. Ensure that the patient's name, address, phone number, sex, date of birth, and relevant prescription numbers are fully filled out.
-
Neglecting to Document the Incident Date: It's crucial to accurately record the date of the error. Omitting this information can hinder the investigation process and make it difficult to track patterns or recurring issues.
-
Misclassifying the Type of Incident: Selecting the wrong type of incident can lead to misunderstandings and mismanagement of the situation. Take the time to carefully consider whether the error was a medication incident or a discrepancy before making a selection.
-
Inadequate Description of the Incident: Providing vague or insufficient details in the description section can leave critical gaps in understanding what went wrong. Be thorough and clear about the facts known at the time of discovery.
-
Failure to Notify Relevant Parties: Not informing the physician or pharmacy manager about the incident can have serious consequences for patient safety. Always ensure that notifications are made promptly and documented appropriately.