Fill in a Valid Immunization Record Form
Document Sample
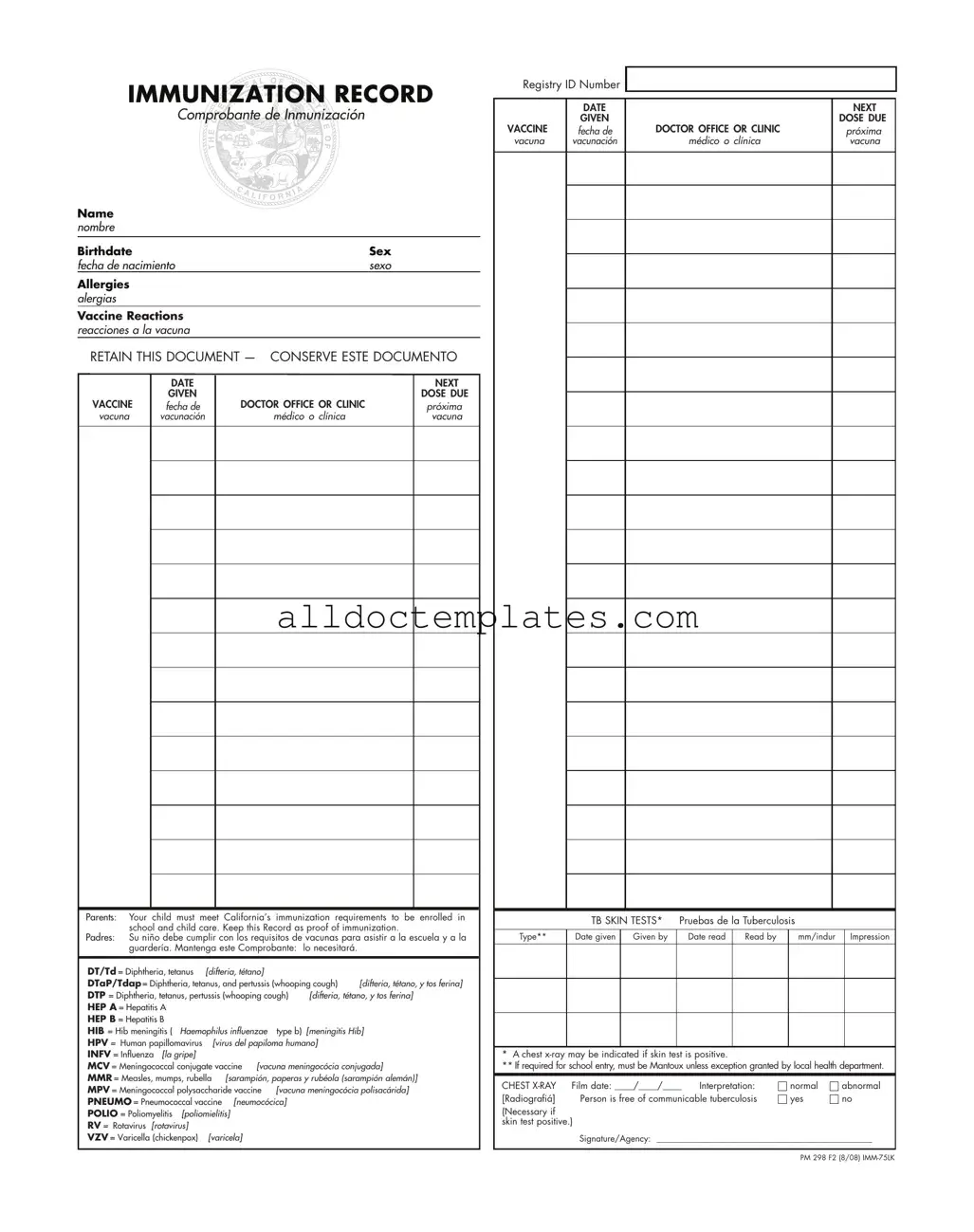
IMMUNIZATION RECORD
Comprobante de Inmunización
Name nombre
Birthdate |
|
|
Sex |
||
fecha de nacimiento |
|
sexo |
|||
Allergies |
|
|
|
|
|
alergias |
|
|
|
|
|
Vaccine Reactions |
|
|
|
|
|
reacciones a la vacuna |
|
|
|
|
|
RETAIN THIS DOCUMENT — CONSERVE ESTE DOCUMENTO |
|||||
|
DATE |
|
|
NEXT |
|
|
|
|
|||
|
GIVEN |
|
|
DOSE DUE |
|
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
|
próxima |
|
vacuna |
vacunación |
médico o clínica |
|
vacuna |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Parents: Your child must meet California’s immunization requirements to be enrolled in school and child care. Keep this Record as proof of immunization.
Padres: Su niño debe cumplir con los requisitos de vacunas para asistir a la escuela y a la guardería. Mantenga este Comprobante: lo necesitará.
DT/Td = Diphtheria, tetanus |
[difteria, tétano] |
|
|
|
|
DTaP/Tdap = Diphtheria, tetanus, and pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
DTP = Diphtheria, tetanus, pertussis (whooping cough) |
[difteria, tétano, y tos ferina] |
||||
HEP A = Hepatitis A |
|
|
|
|
|
HEP B = Hepatitis B |
|
|
|
|
|
HIB = Hib meningitis ( |
Haemophilus influenzae |
type b) |
[meningitis Hib] |
||
HPV = Human papillomavirus |
[virus del papiloma humano] |
|
|||
INFV = Influenza [la gripe] |
|
|
|
|
|
MCV = Meningococcal conjugate vaccine [vacuna meningocócia conjugada] |
|||||
MMR = Measles, mumps, rubella [sarampión, paperas y rubéola (sarampión alemán)] |
|||||
MPV = Meningococcal polysaccharide vaccine |
[vacuna meningocócia polisacárida] |
||||
PNEUMO = Pneumococcal vaccine [neumocócica] |
|
|
|||
POLIO = Poliomyelitis |
[poliomielitis] |
|
|
|
|
RV = Rotavirus [rotavirus] |
|
|
|
|
|
VZV = Varicella (chickenpox) |
[varicela] |
|
|
|
|
Registry ID Number
|
DATE |
|
NEXT |
|
GIVEN |
|
DOSE DUE |
VACCINE |
fecha de |
DOCTOR OFFICE OR CLINIC |
próxima |
vacuna |
vacunación |
médico o clínica |
vacuna |
|
TB SKIN TESTS* |
Pruebas de la Tuberculosis |
|
|
|||
|
|
|
|
|
|
|
|
Type** |
Date given |
Given by |
Date read |
Read by |
|
mm/indur |
Impression |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* A chest
** If required for school entry, must be Mantoux unless exception granted by local health department.
CHEST |
Film date: ____/____/____ |
Interpretation: |
|
normal |
|
abnormal |
|
[Radiografiá] |
Person is free of communicable tuberculosis |
|
yes |
|
|
no |
|
|
|
|
|||||
(Necessary if skin test positive.)
Signature/Agency: __________________________________________________
PM 298 F2 (8/08)
Document Information
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Immunization Record form serves as proof of a child's vaccinations, which is essential for enrollment in schools and child care facilities in California. |
| California Governing Law | California Education Code Section 49403 mandates that children must meet specific immunization requirements before they can attend school or child care. |
| Retention of Document | Parents are advised to keep this record safe, as it may be needed for future school enrollments or medical purposes. |
| Vaccination Types | The form includes various vaccines such as DTaP, MMR, and HPV, ensuring comprehensive immunization against common diseases. |
Immunization Record - Usage Guidelines
Completing the Immunization Record form is an important step in ensuring your child meets the necessary health requirements for school and childcare enrollment. Follow these steps carefully to fill out the form accurately.
- Name: Enter your child's full name in the designated field.
- Birthdate: Fill in your child's date of birth.
- Sex: Indicate your child's sex by selecting the appropriate option.
- Allergies: List any known allergies your child has.
- Vaccine Reactions: Note any previous reactions your child has had to vaccines.
- Date: Write the date of the vaccination in the provided space.
- Next Dose Due: Indicate when the next vaccination is due.
- Vaccine: Select the type of vaccine administered from the list provided.
- Doctor's Office or Clinic: Enter the name of the healthcare provider or clinic where the vaccine was given.
- Registry ID Number: If applicable, fill in the registry ID number.
- TB Skin Tests: If your child has undergone a TB skin test, provide the type, date given, who administered it, date read, and the results.
- Chest X-Ray: If required, enter the film date and interpretation results.
- Signature/Agency: Sign the form and include the name of the agency if applicable.
Once you have completed the form, keep it in a safe place as it serves as proof of your child's immunization status. You may need to present it for school enrollment or childcare purposes.
Common PDF Forms
Chick - Specify your available hours for scheduling purposes.
When dealing with the sale of a mobile home, it is essential to have the proper documentation in place to prevent misunderstandings. The Virginia Mobile Home Bill of Sale form is integral to this process, as it encapsulates all necessary information about the transaction. For those looking to create or obtain this document, a helpful resource can be found at https://mobilehomebillofsale.com/blank-virginia-mobile-home-bill-of-sale, which provides a blank template specifically designed for Virginia. Ensuring that both parties thoroughly complete this form will help streamline the transfer and safeguard the interests of everyone involved.
1099 Nec Fillable Form - If you have questions about your 1099-NEC, consider consulting a tax professional.
Dos and Don'ts
When filling out the Immunization Record form, it’s important to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn’t do:
- Do provide accurate information about your child’s name and birthdate.
- Do list any allergies your child has clearly.
- Do keep the record in a safe place for future reference.
- Do ensure that the vaccine dates are filled in correctly.
- Do have the form signed by the healthcare provider administering the vaccines.
- Don’t leave any sections blank; fill out all required fields.
- Don’t use abbreviations that may confuse others reviewing the form.
- Don’t forget to check for any required signatures or stamps.
- Don’t submit the form without reviewing it for errors.
- Don’t overlook the importance of keeping this document for school enrollment.
Common mistakes
-
Incomplete Information: Failing to fill in all required fields, such as name, birthdate, or allergies, can lead to delays in processing. Ensure every section is completed accurately.
-
Incorrect Vaccine Dates: Entering the wrong dates for vaccinations can cause confusion. Double-check the dates to ensure they align with your child's immunization schedule.
-
Omitting Doctor's Information: Not providing the name of the doctor or clinic administering the vaccines can hinder verification. Always include this information for proper record-keeping.
-
Neglecting to Keep a Copy: Failing to retain a copy of the immunization record for personal files can lead to issues in the future. Keep this document safe as proof of immunization.
-
Ignoring Allergies and Reactions: Not disclosing any known allergies or past vaccine reactions can pose health risks. Always provide this information to ensure your child's safety.