Fill in a Valid Alabama High School Physical Form
Document Sample

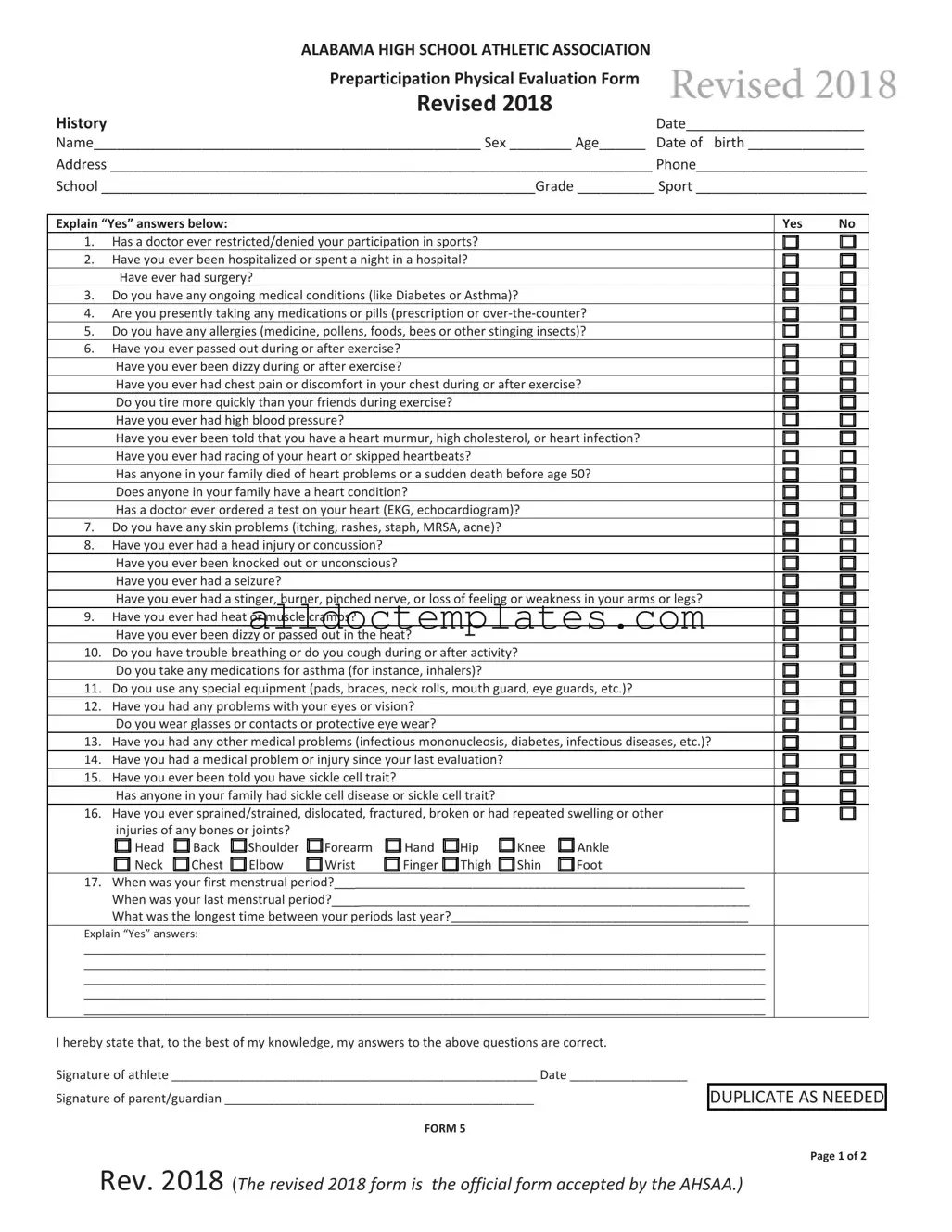
ALABAMA HIGH SCHOOL ATHLETIC ASSOCIATION |
Revised 2018 |
Revised 2018 |
|
Preparticipation Physical Evaluation Form |
|
History |
Date_______________________ |
Name__________________________________________________ Sex ________ Age______ Date of birth _______________
Address ______________________________________________________________________ Phone______________________
School ________________________________________________________Grade __________ Sport ______________________
Explain “Yes” answers below: |
|
|
|
|
|
Yes |
No |
||||
1. |
Has a doctor ever restricted/denied your participation in sports? |
|
|
|
|
|
|||||
2. |
Have you ever been hospitalized or spent a night in a hospital? |
|
|
|
|
|
|||||
|
Have ever had surgery? |
|
|
|
|
|
|
|
|
||
3. |
Do you have any ongoing medical conditions (like Diabetes or Asthma)? |
|
|
|
|
||||||
4. |
Are you presently taking any medications or pills (prescription or over‐the‐counter? |
|
|||||||||
5. |
Do you have any allergies (medicine, pollens, foods, bees or other stinging insects)? |
|
|||||||||
6. |
Have you ever passed out during or after exercise? |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|||||
|
Have you ever been dizzy during or after exercise? |
|
|
|
|
|
|
|
|||
|
Have you ever had chest pain or discomfort in your chest during or after exercise? |
|
|||||||||
|
Do you tire more quickly than your friends during exercise? |
|
|
|
|
|
|
||||
|
Have you ever had high blood pressure? |
|
|
|
|
|
|
|
|||
|
Have you ever been told that you have a heart murmur, high cholesterol, or heart infection? |
|
|||||||||
|
Have you ever had racing of your heart or skipped heartbeats? |
|
|
|
|
|
|||||
|
Has anyone in your family died of heart problems or a sudden death before age 50? |
|
|||||||||
|
Does anyone in your family have a heart condition? |
|
|
|
|
|
|
||||
|
Has a doctor ever ordered a test on your heart (EKG, echocardiogram)? |
|
|
|
|
||||||
7. |
Do you have any skin problems (itching, rashes, staph, MRSA, acne)? |
|
|
|
|
|
|||||
8. |
Have you ever had a head injury or concussion? |
|
|
|
|
|
|
|
|||
|
Have you ever been knocked out or unconscious? |
|
|
|
|
|
|
|
|||
|
Have you ever had a seizure? |
|
|
|
|
|
|
|
|
||
|
Have you ever had a stinger, burner, pinched nerve, or loss of feeling or weakness in your arms or legs? |
|
|||||||||
9. |
Have you ever had heat or muscle cramps? |
|
|
|
|
|
|
|
|||
|
Have you ever been dizzy or passed out in the heat? |
|
|
|
|
|
|
||||
10. Do you have trouble breathing or do you cough during or after activity? |
|
|
|
|
|||||||
|
Do you take any medications for asthma (for instance, inhalers)? |
|
|
|
|
|
|||||
11. Do you use any special equipment (pads, braces, neck rolls, mouth guard, eye guards, etc.)? |
|
||||||||||
12. Have you had any problems with your eyes or vision? |
|
|
|
|
|
|
|||||
|
Do you wear glasses or contacts or protective eye wear? |
|
|
|
|
|
|
||||
13. Have you had any other medical problems (infectious mononucleosis, diabetes, infectious diseases, etc.)? |
|
||||||||||
14. Have you had a medical problem or injury since your last evaluation? |
|
|
|
|
|
||||||
15. Have you ever been told you have sickle cell trait? |
|
|
|
|
|
|
|
||||
|
Has anyone in your family had sickle cell disease or sickle cell trait? |
|
|
|
|
|
|||||
16. Have you ever sprained/strained, dislocated, fractured, broken or had repeated swelling or other |
|
||||||||||
|
injuries of any bones or joints? |
|
|
|
|
|
|
|
|
||
|
Head |
Back |
Shoulder |
Forearm |
Hand |
Hip |
Knee |
Ankle |
|
||
|
Neck |
Chest |
Elbow |
Wrist |
Finger |
Thigh |
Shin |
Foot |
|
||
17.When was your first menstrual period?__________________________________________________________________
When was your last menstrual period?___________________________________________________________________
What was the longest time between your periods last year?________________________________________________
Explain “Yes” answers:
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
______________________________________________________________________________________________________________
I hereby state that, to the best of my knowledge, my answers to the above questions are correct.
Signature of athlete ___________________________________________________________ Date ___________________
Signature of parent/guardian __________________________________________________
FORM 5
DUPLICATE AS NEEDED
Rev. 2018 (The revised 2018 form is the official form accepted by the AHSAA.)
Page 1 of 2
Preparticipation Physical Evaluation Rule 1, Sec. 14 — In order for a student to be eligible for interscholastic athletics, there must be
on file in the Superintendent’s or Principal’s office a current physician’s statement certifying that
__________________________________________ the student has passed a physical exam, and that in the opinion of the examining physician (M.D.
|
|
|
Student's name |
or D.O.) the student is fully able to participate in interscholastic athletics (Grade s 7‐12). The |
||||
|
|
|
AHSAA Physicians Certificate (Form 5 Rev. 2018) must be used. A physical exam will satisfy the |
|||||
|
|
|
|
|
||||
Physical Examination |
requirement for one calendar year through the end of the month from the date of the exam. For |
|||||||
example, a physical given on May 5, 2019, will satisfy the requirement through May 31, 2020. |
||||||||
|
|
|
|
|
|
|
||
|
|
|
Height ____________ Weight _____________ BP _____ / _____ Pulse ____________ |
|
||||
|
|
|
Vision R 20 / ____ L 20 / ____ Corrected: Y N |
Revised 2018 |
|
|||
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
LIMITED |
|
Normal |
|
|
Abnormal Findings |
|
|
|
|
|
|
|
|
|
|
|
|
Cardiovascular |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pulses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E.N.T. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE |
|
Abdominal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Genitalia (males) |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Musculoskeletal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neck |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shoulder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Elbow |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wrist |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hand |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Back |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Knee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ankle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Foot |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Clearance:
A.Cleared
B.Cleared after completing evaluation/rehabilitation for: _______________________________________
C. Not cleared for: |
Collision |
|
|
|
Contact |
|
|
|
Noncontact ____ Strenuous |
____ Moderately strenuous |
____ Nonstrenuous |
Due to: ____________________________________________________________________________________________
Recommendation: _________________________________________________________________________________________
________________________________________________________________________________________________________
________________________________________________________________________________________________________
Name of physician ________________________________________________________________ Date ____________________
Address ________________________________________________________________________ Phone___________________
.
Signature of physician _____________________________________________________________, M.D. or D.O.
(Form must be signed and dated by the attending physician.)
Rev. 2018 (The revised 2018 form is the official form accepted by the AHSAA.)
Document Information
| Fact Name | Details |
|---|---|
| Governing Law | The Alabama High School Athletic Association (AHSAA) Rule 1, Sec. 14 mandates that a current physician's statement must be on file for student-athletes. |
| Eligibility Requirement | Students in grades 7-12 must pass a physical exam to be eligible for interscholastic athletics. |
| Form Usage | The AHSAA Physicians Certificate (Form 5) is the required document to certify a student's physical exam. |
| Physical Exam Validity | A physical exam is valid for one calendar year from the date of the exam. |
| Evaluation Findings | Physicians can clear students for participation, require rehabilitation, or deny clearance based on their evaluation. |
| Information Collected | The form collects personal information, medical history, and details about previous injuries or conditions. |
Alabama High School Physical - Usage Guidelines
Filling out the Alabama High School Physical form is an important step in ensuring that a student athlete is ready for participation in sports. This process involves providing personal information, answering medical history questions, and obtaining a physician's evaluation. Following the steps carefully will help ensure that all necessary information is accurately captured.
- Gather Necessary Information: Before starting the form, collect the athlete's personal details, including name, age, address, school, and grade.
- Complete the Medical History Section: Answer all questions regarding past medical issues, injuries, and current health conditions. Be honest and thorough in your responses.
- Detail Any "Yes" Responses: If any questions in the medical history section are answered with "Yes," provide explanations in the space provided. Include details about the condition, dates, and any treatments received.
- Provide Contact Information: Fill in the athlete's date of birth and phone number. This information is crucial for emergency contact purposes.
- Sign the Form: The athlete should sign and date the form to affirm that all information is accurate. A parent or guardian must also sign and date the form, acknowledging the information provided.
- Schedule a Physical Examination: Take the completed form to a physician (M.D. or D.O.) for a physical examination. The physician will complete the evaluation section of the form.
- Physician's Certification: Ensure the physician signs and dates the form, indicating whether the athlete is cleared for participation in sports.
- Submit the Form: Once completed, submit the signed form to the school’s Superintendent or Principal’s office. This should be done before the athlete can participate in any interscholastic athletics.
Common PDF Forms
Which of These Items Is Checked in a Pre-trip Inspection - Check the brakes for responsiveness and noise.
Lic Forms - Timely updates on personnel changes reflect positively on facility management.
When navigating the complexities of divorce, having a solid understanding of the Colorado Divorce Settlement Agreement form is essential, as it encompasses important elements like property division and child custody arrangements. For those seeking assistance in this process, resources such as Colorado PDF Templates can provide valuable guidance and templates to ensure a smooth transition during this challenging time.
Da 5960 Army - By filing the DA 5960, service members can advocate for their financial rights and responsibilities.
Dos and Don'ts
When filling out the Alabama High School Physical form, it is essential to follow specific guidelines to ensure accuracy and compliance. Here are seven things you should and shouldn't do:
- Do provide accurate personal information, including your name, age, and address.
- Do answer all medical history questions truthfully, including any past injuries or conditions.
- Do have a parent or guardian review the form before submission if you are under 18.
- Do ensure that the physician's signature is included and dated.
- Don't leave any sections blank; all questions must be answered.
- Don't forge signatures or provide false information, as this can lead to disqualification.
- Don't forget to make a copy of the completed form for your records.
Common mistakes
-
Incomplete Personal Information: Failing to provide complete personal details such as name, age, and address can lead to delays in processing the form. It is essential to ensure that all sections are filled out accurately.
-
Neglecting Medical History: Omitting past medical conditions or injuries can jeopardize the athlete's safety. It is crucial to disclose any history of concussions, surgeries, or chronic conditions.
-
Incorrect Signatures: The form requires signatures from both the athlete and a parent or guardian. Missing one of these signatures can render the form invalid.
-
Failure to Update Information: Submitting an outdated physical examination can result in ineligibility for participation. Athletes must ensure that the physical is current, as it is valid for only one calendar year.
-
Ignoring Additional Instructions: Not following specific instructions regarding the physical examination or additional documentation can lead to complications. Athletes should carefully read and adhere to all guidelines provided on the form.