Fill in a Valid 680 Form
Document Sample

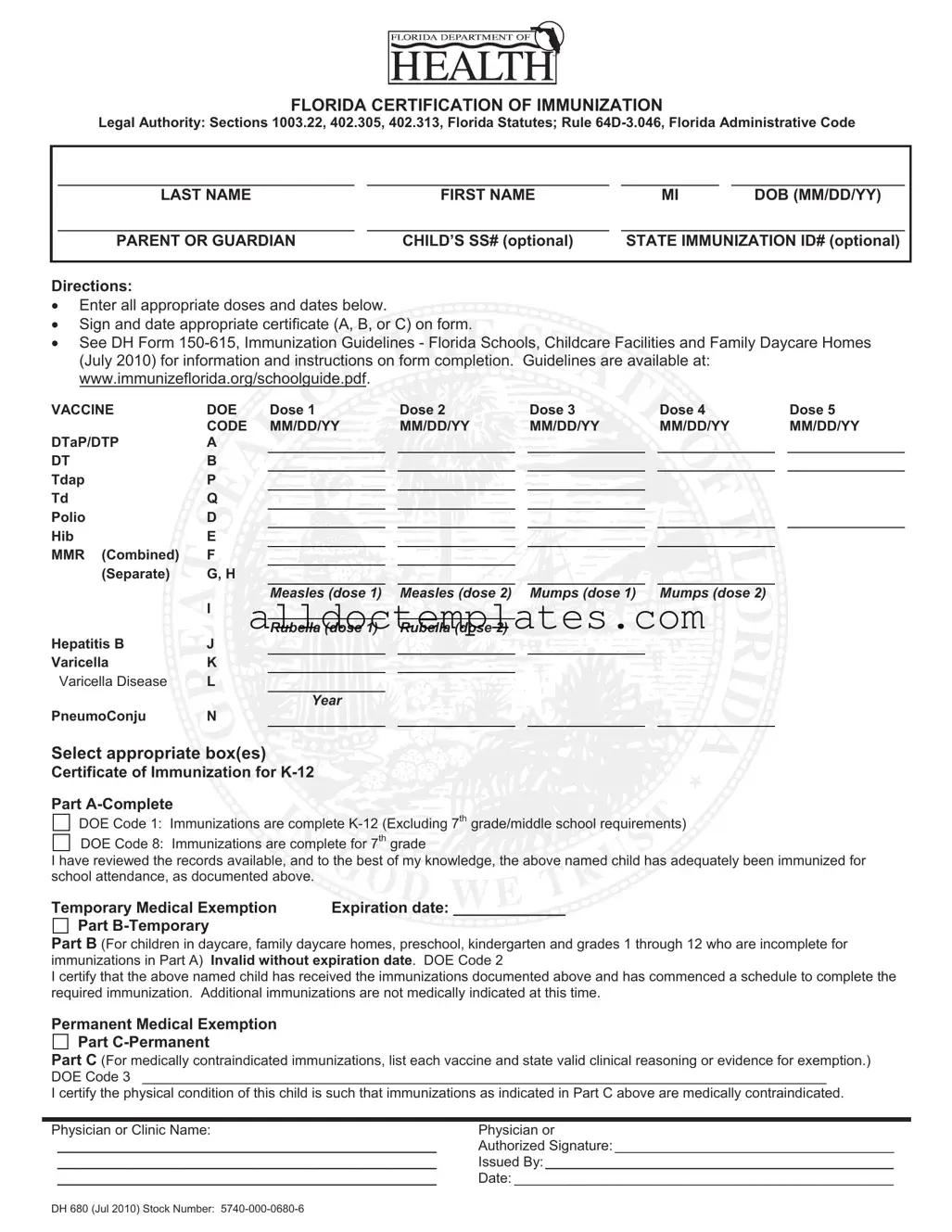
FLORIDA CERTIFICATION OF IMMUNIZATION
Legal Authority: Sections 1003.22, 402.305, 402.313, Florida Statutes; Rule
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
FIRST NAME |
|
MI |
|
DOB (MM/DD/YY) |
|
|
|
|
|
|
|
|
|
|
|
PARENT OR GUARDIAN |
|
CHILD’S SS# (optional) |
|
STATE IMMUNIZATION ID# (optional) |
|
||
|
|
|
|
|
|
|
|
|
Directions:
Enter all appropriate doses and dates below.
Sign and date appropriate certificate (A, B, or C) on form.
or C) on form.
See DH Form 










VACCINE |
DOE |
Dose 1 |
|
Dose 2 |
|
Dose 3 |
|
Dose 4 |
|
Dose 5 |
|
CODE |
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
|
MM/DD/YY |
DTaP/DTP |
A |
|
|
|
|
|
|
|
|
|
DT |
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Tdap |
P |
|
|
|
|
|
|
|
|
|
Td |
Q |
|
|
|
|
|
|
|
|
|
Polio |
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Hib |
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MMR (Combined) |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
(Separate) |
G, H |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Measles (dose 1) |
|
Measles (dose 2) |
|
Mumps (dose 1) |
|
Mumps (dose 2) |
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rubella (dose 1) |
|
Rubella (dose 2) |
|
|
|
|
|
|
Hepatitis B |
J |
|
|
|
|
|
|
|
|
|
Varicella |
K |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Varicella Disease |
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year
PneumoConju N
Select appropriate box(es)
box(es)
Certificate of Immunization  K-12
K-12
Part
DOE Code 1: Immunizations are complete
DOE Code 8: Immunizations are complete for 7th grade
are complete for 7th grade
I have reviewed the records available, and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.
and to the best of my knowledge, the above named child has adequately been immunized for school attendance, as documented above.


Temporary Medical Exemption |
Expiration date: _____________ |
Part |
|
Part B (For children in daycare, family daycare homes, preschool, kindergarten and grades 1 through 12 who are incomplete for immunizations in Part A) Invalid without expiration date. DOE Code 2
I certify that the above named child has received the immunizations documented above and has commenced a schedule to complete the required immunization. Additional immunizations are not medically indicated at this time.
Permanent Medical Exemption
Part
Part C (For medically contraindicated immunizations, list each vaccine and state valid clinical reasoning or evidence for exemption.) DOE Code 3 ________________________________________________________________________________________
I certify the physical condition of this child is such that immunizations as indicated in Part C above are medically contraindicated.
Physician or Clinic Name: |
Physician or |
_________________________________________________ |
Authorized Signature: ____________________________________ |
_________________________________________________ |
Issued By:_____________________________________________ |
_________________________________________________ |
Date: _________________________________________________ |
DH 680 (Jul 2010) Stock Number:
Document Information
| Fact Name | Description |
|---|---|
| Legal Authority | The 680 form is governed by Sections 1003.22, 402.305, and 402.313 of the Florida Statutes, as well as Rule 64D-3.046 of the Florida Administrative Code. |
| Purpose | This form certifies that a child has received the necessary immunizations required for school attendance in Florida. |
| Optional Information | Parents can provide the child's Social Security number and State Immunization ID number, but these are not mandatory. |
| Immunization Documentation | All doses and dates of vaccines must be entered on the form to ensure compliance with immunization requirements. |
| Temporary Medical Exemption | Part B of the form allows for a temporary medical exemption, which must include an expiration date to be valid. |
| Permanant Medical Exemption | Part C provides a space for permanent medical exemptions, requiring a valid clinical reason for each exemption listed. |
| Review Requirement | The form requires a review of the child's immunization records by a physician or authorized clinic representative. |
| Issuance Date | The form is identified as DH 680 and was last updated in July 2010. |
680 - Usage Guidelines
Completing the Florida Certification of Immunization Form 680 is an essential step for ensuring that a child meets the immunization requirements for school attendance. The form requires specific information about the child and their immunization history. After filling out the form, it will need to be signed by a healthcare provider to verify the information provided.
- Begin by entering the child’s last name, first name, and middle initial in the designated fields.
- Input the child’s date of birth in the format MM/DD/YY.
- Provide the name of the parent or guardian.
- If available, enter the child’s Social Security number and state immunization ID number in the optional fields.
- In the section labeled VACCINE, list the vaccines administered by entering the appropriate doses and dates in the corresponding fields.
- For each vaccine, fill in the dose number and the date administered for doses 1 through 5.
- After completing the vaccine section, select the appropriate certificate box (A, B, or C) based on the child’s immunization status.
- If applicable, provide the expiration date for any temporary medical exemptions.
- For Part C, if the child has a permanent medical exemption, list each vaccine and the valid clinical reasoning for the exemption.
- Finally, have the form signed by a physician or authorized healthcare provider, and ensure their name and the date are clearly indicated.
Common PDF Forms
Where Is Depreciation on Tax Return - This form represents the bridge between various forms of income and the overarching individual tax return.
For those looking to navigate the intricacies of mobile home transactions, it is essential to utilize the appropriate documentation such as the Virginia Mobile Home Bill of Sale. This document not only facilitates the transfer of ownership but also serves as a critical safeguard for both buyer and seller. To access a reliable template for this important form, you can visit mobilehomebillofsale.com/blank-virginia-mobile-home-bill-of-sale/, ensuring that you have all necessary information covered.
Bracket Pdf - The tournament typically features 68 teams competing for the title.
Employment Verification Form - The I-9 form assists in ensuring that workers are legally authorized to work in the U.S.
Dos and Don'ts
When filling out the Florida Certification of Immunization (Form 680), consider the following guidelines to ensure accuracy and compliance.
- Do provide complete and accurate information for the child’s name, date of birth, and parent or guardian details.
- Do enter all appropriate vaccine doses and dates clearly in the designated spaces.
- Do sign and date the appropriate certificate (A, B, or C) at the end of the form.
- Do review the immunization records thoroughly before submission.
- Don't leave any sections blank; all relevant information must be filled out.
- Don't forget to include the expiration date for any temporary medical exemptions.
- Don't use abbreviations or shorthand that may confuse the reader.
- Don't submit the form without verifying that all information is accurate and complete.
Common mistakes
-
Failing to provide the child's full name, including last name, first name, and middle initial. This information is essential for proper identification.
-
Not including the date of birth in the correct format (MM/DD/YY). Incorrect formatting can lead to confusion and delays.
-
Leaving out the parent or guardian's name. This information is necessary for contact purposes and verification.
-
Neglecting to fill in the immunization dates accurately. Each dose must have a corresponding date to validate the immunization schedule.
-
Not signing or dating the appropriate certificate (A, B, or C). A signature is required to confirm the accuracy of the information provided.
-
Using the wrong DOE code. Selecting the incorrect code can misrepresent the child's immunization status.
-
Failing to check for the expiration date on temporary medical exemptions. An exemption without a date is invalid.